-
 30,000+ Students Sucessfully Trained Annually
30,000+ Students Sucessfully Trained Annually
-
30,000+ Students Sucessfully Trained Annually
Every year, hundreds of thousands of people experience cardiac arrest, a life-threatening emergency in which the heart suddenly stops pumping blood effectively. When cardiac arrest occurs, blood flow to the brain and other vital organs ceases, causing the person to become unresponsive and stop breathing normally. Common causes include acute myocardial infarction, severe arrhythmias, respiratory failure, trauma, electrolyte abnormalities, and other underlying medical conditions. Without immediate intervention, cardiac arrest can rapidly result in death.
The Adult Cardiac Arrest Algorithm is a structured, evidence-based approach developed by the American Heart Association (AHA) to guide healthcare providers during resuscitation. The algorithm emphasizes rapid recognition, initiation of high-quality CPR, rhythm assessment using a monitor/defibrillator, timely defibrillation for shockable rhythms, appropriate medication administration, advanced airway management when indicated, and identification of reversible causes. By following this systematic process, healthcare teams can improve the likelihood of return of spontaneous circulation (ROSC) and increase survival rates.
Note: This adult cardiac arrest algorithm guideline remains valid for the period 2025–2030.

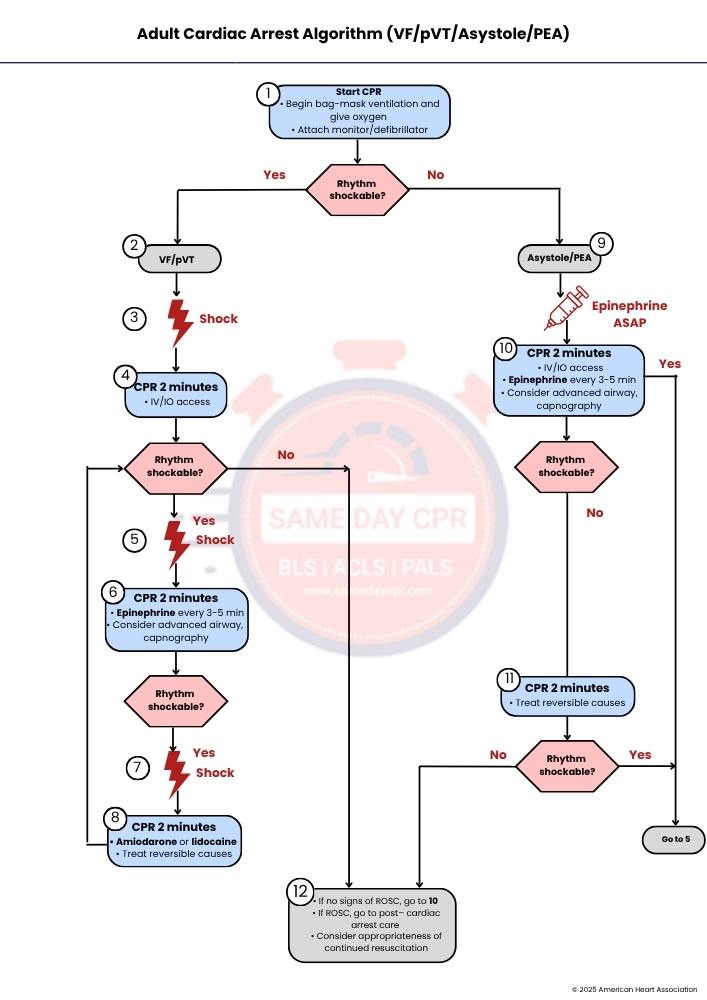
Begin high-quality CPR immediately to maintain blood flow to the brain and heart. Start bag-mask ventilation and give 100% oxygen to support breathing. Quickly attach a monitor/defibrillator to identify the heart rhythm. After rhythm analysis, decide the next step: if the rhythm is shockable (ventricular fibrillation or pulseless ventricular tachycardia), proceed to Step 2. If the rhythm is not shockable (asystole or pulseless electrical activity), skip the shock pathway and go to Step 9. Early CPR and rapid rhythm recognition are critical because survival depends on minimizing interruptions in chest compressions.
This step identifies a shockable rhythm: ventricular fibrillation (VF) or pulseless ventricular tachycardia (pVT). These rhythms indicate chaotic or very fast electrical activity where the heart cannot pump blood effectively. Once confirmed, the immediate priority is defibrillation because electrical shock is the most effective way to reset the heart’s rhythm. At this stage, CPR should continue with minimal delay while preparing to deliver the shock.
Deliver an immediate defibrillation shock as soon as the defibrillator is ready. This is aimed at stopping the abnormal electrical activity so the heart’s normal pacemaker can restart an organized rhythm. After the shock, do not pause for rhythm checks or pulse checks—resume CPR right away to maintain circulation. Quick shock delivery is essential because delays significantly reduce the chance of successful resuscitation.
After the shock, resume high-quality CPR for 2 minutes without interruption. During this cycle, establish IV or IO access to give medications and fluids. After 2 minutes, reassess the rhythm. If the rhythm remains shockable, proceed to Step 5. If it becomes non-shockable, switch to Step 12 for further evaluation and treatment. Continuous CPR helps maintain coronary and cerebral perfusion between shocks.
If the rhythm is still VF or pVT after the CPR cycle, deliver another defibrillation shock. This repeated shock strategy increases the likelihood of terminating the abnormal electrical activity. Immediately resume CPR after the shock for another 2-minute cycle. Each shock is followed by CPR to support circulation and improve the effectiveness of subsequent defibrillation attempts.
Continue CPR for 2 minutes while giving epinephrine every 3 to 5 minutes to improve blood flow to the heart and brain by constricting blood vessels. Consider placing an advanced airway (such as an endotracheal tube) and using capnography to monitor ventilation and CPR quality. After 2 minutes, reassess the rhythm. If still shockable, proceed to Step 7. If non-shockable, move to Step 12. This step combines medications and advanced airway management to support resuscitation efforts.
If VF or pVT persists, deliver another shock immediately. This continues the cycle of defibrillation and CPR, aiming to terminate the abnormal rhythm. After the shock, resume CPR right away for 2 minutes. Repeated shocks combined with medications increase the chances of achieving return of spontaneous circulation (ROSC).
Continue CPR for 2 minutes while administering antiarrhythmic medications such as amiodarone or lidocaine to stabilize the heart’s electrical activity and prevent recurrent arrhythmias. At the same time, actively search for and treat reversible causes (the H’s and T’s, such as hypoxia, hypovolemia, tension pneumothorax, or tamponade). Addressing underlying causes is critical for long-term success. Continue cycles until rhythm changes or ROSC occurs.
If the rhythm is asystole or pulseless electrical activity (PEA), this is a non-shockable rhythm. Immediate administration of epinephrine is recommended as soon as possible to improve perfusion and support cardiac activity. CPR should continue without interruption. At this stage, focus shifts away from defibrillation and toward medication, high-quality compressions, and identifying reversible causes.
Continue CPR for 2 minutes while establishing IV or IO access. Give epinephrine every 3 to 5 minutes to support circulation. Consider placing an advanced airway and using capnography to ensure adequate ventilation and CPR quality. After 2 minutes, reassess rhythm: if it becomes shockable, go to Step 5. If still non-shockable, proceed to Step 11. This step emphasizes ongoing medication and advanced support in non-shockable cardiac arrest.
Continue CPR for 2 minutes while actively treating reversible causes (H’s and T’s), such as hypoxia, acidosis, electrolyte imbalance, or thrombosis. After each cycle, reassess the rhythm. If it becomes shockable, move to Step 5 for defibrillation. If it remains non-shockable, proceed to Step 12. This step focuses on identifying and correcting underlying problems that are preventing recovery.
If no signs of return of spontaneous circulation (ROSC), continue resuscitation by returning to Step 10 and repeating the cycle. If ROSC is achieved, transition immediately to post–cardiac arrest care, including airway management, oxygenation, blood pressure support, ECG evaluation, and targeted temperature management if indicated. At this stage, also consider whether continued resuscitation is appropriate based on clinical context, downtime, and patient condition. This step ensures ongoing reassessment and appropriate transition between active resuscitation and post-arrest care.
High-quality CPR is the foundation of adult cardiac arrest care and helps maintain blood flow to vital organs. It requires coordinated teamwork to deliver effective compressions and ventilation without unnecessary delays.
Defibrillation uses an electric shock to help restore a normal heart rhythm during cardiac arrest. Selecting the correct energy level improves the chance of success and supports effective resuscitation.
Medicines play an important role during cardiac arrest and support the heart and circulation. They help improve rhythm control and blood flow while the team continues resuscitation.
Airway management is a key step during cardiac arrest care to keep oxygen moving to the lungs. It helps the team maintain steady breathing support while focusing on high-quality chest compressions.
Cardiac arrest in adults can happen because of problems that we can often fix if we act fast. Doctors look for specific reversible causes called Hs and Ts to quickly find and treat what stopped the heart.
| H’s (Reversible Physiologic Causes) | T’s (Reversible Mechanical/Toxin Causes) |
|---|---|
| Hypovolemia: Low blood volume (severe bleeding or dehydration). Needs fluids or blood. | Tension pneumothorax: Air trapped in the chest compresses the lungs and heart. Requires emergency decompression. |
| Hypoxia: Low oxygen levels. Requires oxygen support or airway correction. | Tamponade, cardiac: Fluid around the heart prevents proper pumping. Needs urgent drainage. |
| Hydrogen ion (acidosis): Too much acid in the blood. Treated by improving breathing and circulation. | Toxins: Poisoning or medicine overdose. Requires antidotes or supportive care. |
| Hypo-/hyperkalemia: Abnormal potassium levels (too low or too high). Can severely affect heart rhythm. | Thrombosis, pulmonary: Blood clot in the lungs (pulmonary embolism). Blocks blood flow. |
| Hypothermia: Body temperature is too low. Needs gradual warming. | Thrombosis, coronary: Heart attack due to blocked coronary arteries. |
In short, cardiac arrest is a sudden and serious emergency that needs fast and organized action to give a person the best chance of survival. The Adult Cardiac Arrest Algorithm guides healthcare providers step-by-step so they can respond quickly, start high-quality CPR, give shocks when needed, and use medicines and airway support in the right way. It also reminds the team to keep checking the heart rhythm, continue compressions with minimal breaks, and look for treatable causes that led to the arrest. When every part of the process works together, blood flow can be restored, and the heart can restart. After recovery, careful follow-up care becomes important to support the patient and improve long-term outcomes.
Enroll in ACLS classes today at Same Day CPR and gain the confidence to take charge in emergencies. This is more than just earning a course completion card—it’s a dedication to saving lives.