-
 30,000+ Students Sucessfully Trained Annually
30,000+ Students Sucessfully Trained Annually
-
30,000+ Students Sucessfully Trained Annually
Imagine a situation where every moment is critical, and two lives depend on a rapid medical response. This is the reality healthcare providers face when cardiac arrest occurs during pregnancy. Although rare, cardiac arrest in pregnancy is one of the most life-threatening emergencies in obstetric care, occurring when a pregnant woman’s heart suddenly stops pumping blood effectively, resulting in loss of consciousness and absence of a pulse. It may arise from pregnancy-related conditions such as severe hemorrhage, preeclampsia/eclampsia, amniotic fluid embolism, or anesthesia complications, as well as non-pregnancy-related causes, including heart disease, trauma, and pulmonary embolism. Because cardiac arrest threatens both maternal and fetal survival, prompt recognition and immediate, specialized resuscitation are essential to improve outcomes for both patients.
The Cardiac Arrest in Pregnancy Algorithm provides a structured approach for healthcare providers to manage maternal cardiac arrest effectively. It emphasizes high-quality cardiopulmonary resuscitation (CPR), early defibrillation when indicated, relief of aortocaval compression by manually displacing the uterus to the left, securing the airway, and identifying reversible causes. The algorithm also guides the team on the timely consideration of a perimortem cesarean delivery (usually within 5 minutes of arrest if resuscitation is unsuccessful) to improve maternal circulation and increase the chances of fetal survival. By following this algorithm, healthcare professionals can deliver coordinated, evidence-based care during this critical emergency.
Note: This cardiac arrest in pregnancy algorithm guideline remains valid for the period 2025–2030.

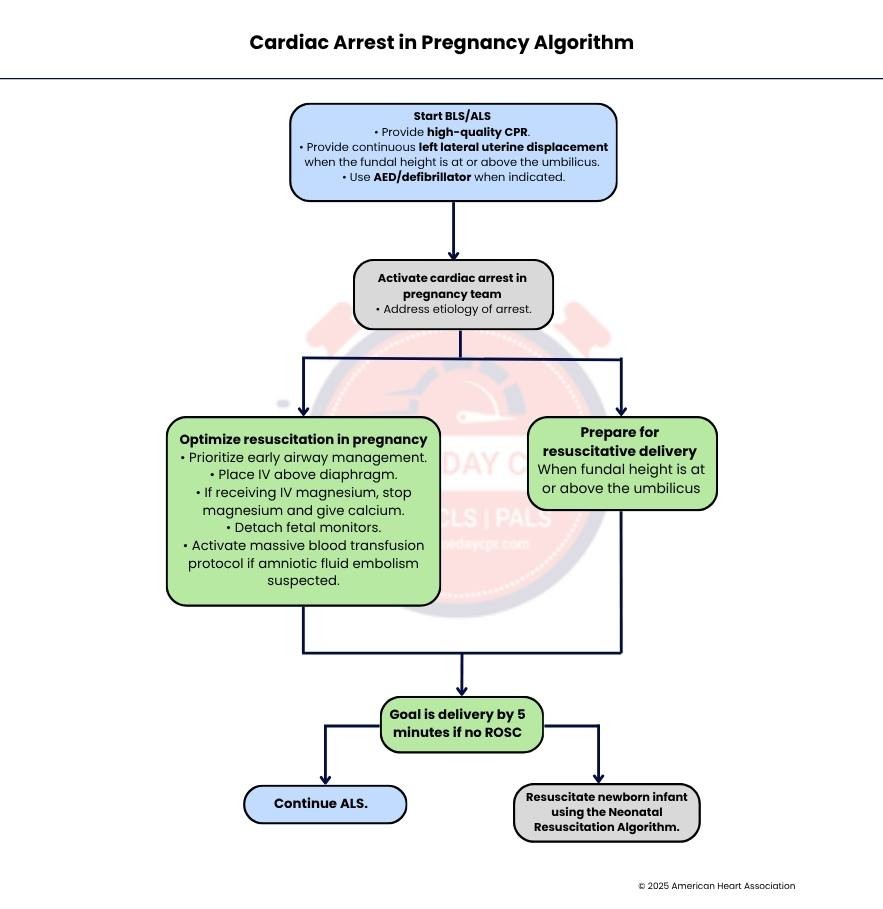
The first step is to begin basic life support (BLS) or advanced life support (ALS) immediately. High-quality CPR should be provided to maintain blood flow to the mother’s vital organs. If the uterus is large enough that the top of it (fundal height) is at or above the level of the umbilicus (belly button), continuous left lateral uterine displacement should be performed to move the uterus away from major blood vessels and improve circulation. An AED or defibrillator should be used if a shockable heart rhythm is present.
As soon as possible, a specialized cardiac arrest in pregnancy team should be activated. The healthcare team should quickly identify and treat the cause of the cardiac arrest. If the pregnant patient requires ongoing resuscitation during pregnancy, the team should move to Step 3. If the cardiac arrest occurs during delivery and resuscitation is needed, the team should proceed directly to Step 6.
Resuscitation efforts should be adjusted to meet the special needs of a pregnant patient. Early airway management should be prioritized to ensure adequate oxygen delivery. Intravenous (IV) access should be placed above the diaphragm to improve medication delivery. If the patient is receiving IV magnesium, it should be stopped, and calcium should be administered because magnesium toxicity can contribute to cardiac arrest. Any fetal monitors should be removed to avoid interference with emergency care. If an amniotic fluid embolism is suspected, a massive blood transfusion protocol should be activated immediately.
The goal at this stage is to achieve delivery within 5 minutes if there is no return of spontaneous circulation (ROSC), meaning the mother's heart has not started beating effectively on its own. Rapid delivery can improve the chances of survival for both the mother and the baby by reducing pressure from the uterus on major blood vessels. If resuscitation is still required after this assessment, proceed to Step 5. If delivery has been completed, proceed to Step 7.
If the patient remains in cardiac arrest, advanced life support measures should continue. This includes ongoing high-quality CPR, airway management, medication administration, rhythm assessment, and treatment according to standard cardiac arrest protocols while addressing any reversible causes.
If cardiac arrest occurs during delivery or if emergency delivery is indicated, preparations for a resuscitative delivery should begin immediately. When the fundal height is at or above the umbilicus, indicating a sufficiently advanced pregnancy, the team should proceed to Step 4 and aim for delivery within 5 minutes if ROSC has not been achieved.
After delivery, the newborn should be assessed and resuscitated according to the Neonatal Resuscitation Algorithm if needed. This process focuses on supporting the infant’s breathing, heart rate, and overall transition to life outside the womb, ensuring that the baby receives appropriate emergency care while maternal resuscitation continues as necessary.
The cardiac arrest team for a pregnant patient may vary depending on the resources available at the hospital. The team usually includes a team leader who coordinates the resuscitation efforts, an anesthesiologist who manages the airway and medications, an obstetrician who provides pregnancy-related care, a neonatologist who cares for the newborn if delivery occurs, nurses who assist with patient monitoring and treatments, pharmacists who prepare and provide medications, and other professionals who may offer additional support as needed.
The goal of left lateral uterine displacement is to move the pregnant uterus away from the large blood vessels in the abdomen. This helps relieve aortocaval compression, which can reduce blood flow to the heart and the rest of the body. Improving blood circulation, it also helps make chest compressions more effective during cardiopulmonary resuscitation (CPR).
The goal of resuscitative delivery is to improve the chances of survival and recovery for the pregnant patient. When possible, it may also improve the outcome for the newborn infant. Delivering the baby can reduce pressure on the mother’s heart and blood vessels, allowing resuscitation efforts to work more effectively.
Ideally, resuscitative delivery should be performed within 5 minutes of maternal cardiac arrest, depending on the resources available at the healthcare facility. Early delivery can improve maternal circulation and increase the likelihood of a successful resuscitation while also giving the newborn a better chance of survival.
In pregnant patients, a difficult airway is common because pregnancy causes changes such as swelling of the airway tissues and increased oxygen demand. Therefore, airway management, including endotracheal intubation or placement of a supraglottic airway, should be performed by the most experienced professional available to ensure the airway is secured quickly and safely.
In short, the Cardiac Arrest in Pregnancy Algorithm gives healthcare teams a clear and organized plan for managing one of the most serious emergencies in obstetric care. By acting quickly, providing high-quality CPR, relieving pressure from major blood vessels, securing the airway, and addressing reversible causes, providers can improve the chances of survival for both the mother and the baby. The algorithm also highlights the importance of timely delivery when resuscitation is not successful, helping support better outcomes during a critical situation. Strong teamwork, effective communication, and careful decision-making are essential throughout the process. Following this evidence-based approach allows healthcare professionals to respond with confidence and provide the best possible care during these time-critical situations.
Advance your emergency cardiovascular care skills with Same Day CPR’s ACLS course. Enroll today to gain the knowledge, hands-on training, and confidence needed to respond effectively in critical cardiac emergencies.