-
 30,000+ Students Sucessfully Trained Annually
30,000+ Students Sucessfully Trained Annually
-
30,000+ Students Sucessfully Trained Annually
When a person’s heart rate feels unusually slow, or when a routine check reveals a low pulse, it raises concerns about what is happening physiologically. Bradycardia with a pulse in adults refers to a condition in which an adult has a slower-than-normal heart rate (typically fewer than 50 beats per minute) while still maintaining an effective, detectable pulse. It can range from being harmless in well-trained athletes to being dangerous when it leads to inadequate blood flow to the body. When bradycardia becomes clinically significant, it can cause symptoms such as dizziness, weakness, shortness of breath, chest discomfort, confusion, or even fainting. The concern is not merely the slow heart rate itself, but whether the slowed cardiac rhythm is able to maintain adequate perfusion of vital organs.
The Adult Bradycardia With a Pulse Algorithm is a structured emergency approach used in advanced cardiac life support (ACLS) to quickly assess and treat symptomatic bradycardia. Its role is to guide healthcare providers through a step-by-step process: first assessing airway, breathing, and circulation, then identifying whether the patient is unstable due to a low heart rate. If the patient shows signs of poor perfusion, the algorithm recommends immediate interventions such as administering atropine, followed by transcutaneous pacing or intravenous infusions like dopamine or epinephrine if atropine is ineffective. The main purpose of the algorithm is to ensure rapid, standardized treatment to prevent cardiac arrest and restore adequate heart function.
Note: This adult bradycardia with a pulse algorithm guideline remains valid for the period 2025–2030.

| Age Group | Normal Heart Rate (beats per minute) | Bradycardia Threshold (beats per minute) |
|---|---|---|
| Adults (18–60 years) | 60–100 | <60 |
| Older Adults (>60 years) | 60–100 | <60 |
Key Points:
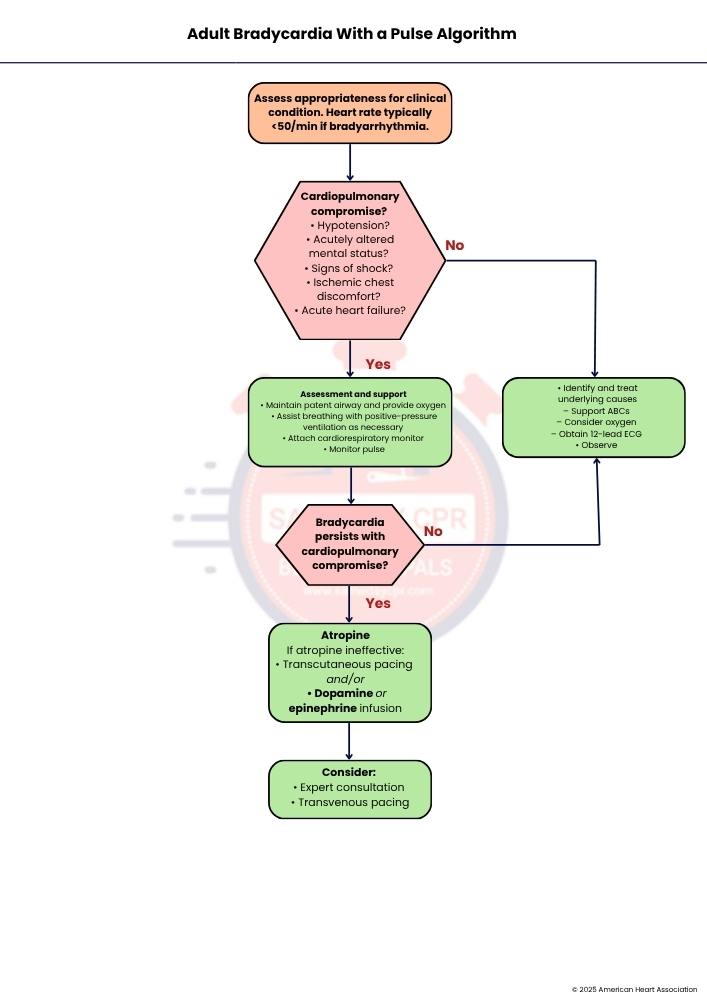
First, determine whether the slow heart rate is appropriate for the patient's condition. Bradyarrhythmia typically refers to a heart rate of less than 50 beats per minute. Assess the patient’s symptoms and overall condition to decide whether the slow heart rate is causing problems and requires treatment.
Check whether the patient is showing signs that the slow heart rate is affecting circulation or breathing. Look for hypotension (low blood pressure), acutely altered mental status, signs of shock, ischemic chest discomfort, or acute heart failure. If any of these signs are present, proceed to Step 3. If none of these signs are present, proceed to Step 7 for monitoring and treatment of underlying causes.
Provide immediate supportive care to stabilize the patient. Maintain a patent airway and provide oxygen when needed. Assist breathing with positive-pressure ventilation if necessary. Attach a cardiorespiratory monitor to continuously observe the patient’s heart rhythm and vital signs, and monitor the pulse closely to detect any changes in the patient’s condition.
After providing initial support, reassess the patient to determine whether bradycardia is still causing cardiopulmonary compromise. If the patient continues to have symptoms or signs of poor circulation despite supportive measures, proceed to Step 5 for additional treatment. If the patient's condition improves and there is no longer evidence of compromise, proceed to Step 7 for continued observation and management.
Administer atropine as the first medication to increase the heart rate. If atropine is ineffective, additional interventions are required. These include transcutaneous pacing, which delivers electrical impulses through the skin to stimulate the heart, and/or a dopamine infusion or epinephrine infusion to improve heart rate and blood pressure. These treatments help maintain adequate circulation until the underlying problem is corrected.
If the patient does not respond adequately to initial treatments, consider obtaining expert consultation for further management. Transvenous pacing is also considered. This procedure involves placing a pacing wire into a vein to provide direct electrical stimulation to the heart and is usually performed when temporary external pacing or medications are not sufficient.
Identify and treat any underlying causes responsible for the bradycardia. Continue to support the airway, breathing, and circulation (ABCs), and consider providing oxygen if needed. Obtain a 12-lead ECG (Electrocardiogram) to evaluate the heart rhythm and look for possible causes. Continue to observe the patient closely and monitor for any changes in condition, ensuring that appropriate treatment is provided if symptoms worsen.
Atropine is the first medication used to treat symptomatic bradycardia. The initial dose is 1 milligram given as an intravenous (IV) bolus. If the slow heart rate persists, the dose is repeated every 3 to 5 minutes. The total amount of atropine given should not exceed 3 milligrams.
Dopamine is used when atropine is ineffective or inappropriate. The usual infusion rate is 5 to 20 micrograms per kilogram per minute. The infusion rate should be adjusted according to the patient’s response, such as improvement in heart rate and blood pressure, and should be reduced gradually when discontinuing treatment.
Epinephrine infusion is another option when atropine does not improve the patient’s condition. It is administered at a rate of 2 to 10 micrograms per minute. The infusion should be titrated according to the patient’s response, with close monitoring to ensure adequate heart rate and blood pressure.
Reduced blood flow to the heart muscle, or a heart attack, can damage the heart’s electrical system and lead to bradycardia. Identifying and treating myocardial ischemia or infarction is important to restore normal heart function and prevent further complications.
Certain medications and toxic substances can slow the heart rate. Drugs such as calcium-channel blockers, beta blockers, and digoxin can cause bradycardia when taken in excessive amounts or when the body reacts strongly to them. Reviewing medications and treating drug toxicity can help correct the problem.
Hypoxia occurs when the body’s tissues do not receive enough oxygen. Low oxygen levels can affect the heart and cause a slow heart rate. Providing oxygen and treating the underlying cause of hypoxia are essential to improve the patient’s condition.
Abnormal levels of electrolytes, especially high potassium levels (hyperkalemia), can interfere with the heart’s electrical activity and lead to bradycardia. Correcting the electrolyte imbalance is important to restore a normal heart rhythm and prevent serious complications.
In short, adult bradycardia with a pulse needs careful attention because a slow heart rhythm can still support the body or signal a serious problem with circulation. The structured algorithm guides healthcare providers to assess the person quickly, focus on breathing and blood flow, and decide if urgent care is needed. It supports clear thinking during stressful moments by encouraging early monitoring and fast recognition of warning signs like low pressure or reduced alertness. When symptoms are present, treatment may include medications to raise the heart rate or electrical pacing when drugs are not enough. Providers also look for underlying causes such as heart injury, medication effects, low oxygen, or electrolyte imbalance, and treat them directly. This organized approach helps restore stable circulation and protects vital organs from harm. With prompt decisions and steady care, outcomes improve, and the risk of serious complications decreases.
Dealing with adult bradycardia or a low pulse in high-pressure situations can be challenging. Same Day CPR’s ACLS courses help physicians, nurses, paramedics, and respiratory therapists build the confidence and skills to manage bradycardia, cardiac emergencies, and more on a schedule that fits your life. Register today and be prepared when it matters.